McFarlane Dental Announces a New Dental Material
McFarlane Dental presents… I am proud to announce that we have added Riva glass ionomer to our offerings of restorative materials. This addition follows the principle of evidence-based dentistry, making decisions based on what research shows is best for patients and long-term outcomes. This material complements our array of restorative options and gives patients a material that is highly rated for it’s strength and handling. The material has been highly rated by Dental Product Shopper, as well as The Dental Advisor, and notably by my friend and colleague Dr. Matt Strepka (of Sandalwood Dental in Houston, TX)
Glass ionomers are biocompatible materials, which can stick (adhere) to tooth structure in difficult to restore areas. The only other material we have in dentistry that is as generous with the exposure to blood and/or saliva is amalgam. The only other white restorative material we have is composite, which is very dense, and very placement sensitive. It is worth noting that as a material glass ionomer has continued to develop; it has improved so markedly from it’s nascency as to become a virtually a new material.
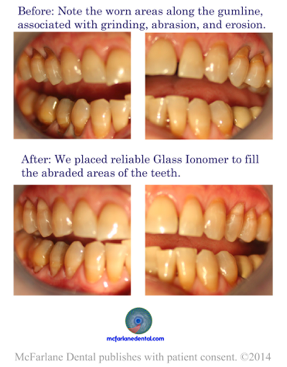
In many patients, you find worn areas at the gumline, which is the result of wear and tear on the teeth. The myriad examples of this type of wear and tear include: grinding, clenching, bruxism, a history of toothbrush abrasion (using a hard brush or an overly aggressive technique), root exposure from recession or bone loss, and erosion caused by an acidic diet or G.E.R.D. These lesions come in many shapes and many forms, but almost none of them come from the traditional caries process. All of the forms of tooth loss that I mention in the list above come from physical and/or chemical wear. Only a small percentage of the gumline cavitation (tooth loss) in the gingival (Class V) gum area come from bacteria emitting acid as a secondary response to a sugary diet. Furthermore, as patients age, the prevalence of recession increases and likewise the weaker areas of the cementum and dentin found in their roots tend to erode away more quickly than their enamel.
Let’s talk briefly about why in cases of erosion, and abrasion in the area of gingival (Class V) fillings glass ionomer is so attractive. Glass ionomer is slightly porous and allows for a more natural biologically compatible integration into the tooth. Glass ionomer allows fluoride to pass through it into tooth, which our other materials do not. For these types of fillings, it is more ideal because it is slightly softer, which means if a person grinds with excessive force causing flexion and abfraction of the tooth, the filling does not chip away at the edges. Glass ionomer does not require any additional preparation of the tooth, which makes it a minimally invasive treatment. Minimally invasive treatment is a hallmark of modern healthcare because it limits the amount of secondary damage being done to repair the tooth.
In (Class V) gingival restorations, composite (being a very durable, dense, and hard material) under abfraction forces of chewing and grinding, which may cause tooth flexure, tend to show signs of chipping at the edges when used in these types of cases. Amalgam has fallen into disfavor within our world for 4 reasons: 1 – it is less aesthetic (it looks silver instead of tooth colored), 2 – it is hard to collect creating a difficult long-term ecological problem, 3 – poorly informed people casting aspersions about it’s safety (while the ADA scientifically-based evidence concluding it is a safe and effective material), and 4 – it requires a minimum 2mm preparation of the tooth with undercut retentive walls so that the filling can be retained (sometimes leading to cracks).
Here is the conclusion of the Dental Research Journal: “In recent decade there has been increasing attention to the use of “smart” bioactive materials in dentistry, especially with the aim of remineralizing dentin… particularly in an attempt to control the prevalence of primary and recurrent caries.” (accessed through NCBI on 9/8/14, http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3793401/)
I am genuinely excited about the addition of this new material and I am making an effort to let people know about it. It is one more small way that we are trying to do the best work we can. 🙂
Sincerely,
J. Russell McFarlane DDS